In the quiet, unspoken dialogue between a nursing mother and her infant lies a biochemical symphony. At the center of this intimate orchestra is oxytocin—a hormone often nicknamed the “love hormone” or “bonding chemical.” It’s what helps mothers release milk during breastfeeding, but more profoundly, it fuels emotional connection. Yet, for many women facing postnatal depression, this natural rhythm seems to falter. A new study published in Psychoneuroendocrinology delves into this delicate relationship, revealing how depression may alter oxytocin’s role—not by reducing its presence, but by breaking its rhythm.
The Hormone Behind the Bond
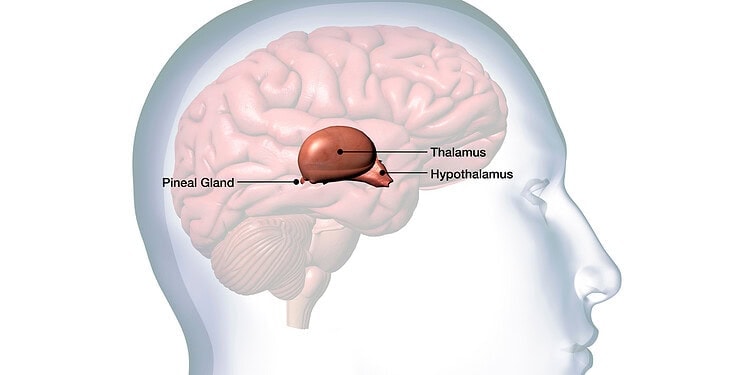
Oxytocin is not just a molecule; it’s a messenger between body and brain, translating physical contact into emotional warmth. During breastfeeding, the hormone is released both peripherally—in the bloodstream to help milk flow—and centrally, in the brain, where it helps forge feelings of calm, reward, and connection. It’s part of an evolutionary design to keep mother and baby tethered through care, touch, and mutual comfort.
Breastfeeding, for many, is more than nutrition. It reduces stress, deepens maternal-infant bonds, and can even serve as a natural buffer against mood disorders. But what happens when that biochemical comfort system falters? For women with postnatal depression—a condition affecting 1 in 5 new mothers—the breastfeeding experience can be marked not by warmth, but by struggle. They report early weaning, emotional detachment, and a gnawing sense of failure. Could the oxytocin system itself be out of sync?
That’s the question researchers set out to investigate.
Unraveling the Mystery: The UCL Study
Led by Kate Lindley Baron-Cohen, a postdoctoral researcher at University College London, the study recruited 62 breastfeeding mothers, aged between 23 and 42, all of whom were 3 to 9 months postpartum. Each mother was asked to complete the Edinburgh Postnatal Depression Scale—a validated measure that screens for depressive symptoms after childbirth. Based on their scores, 26 participants were identified as having probable postnatal depression, while 36 served as a non-depressed comparison group.
But this wasn’t just a psychological survey. The researchers were after something more tangible: the hormonal fingerprints in breast milk. Across three lab sessions, the mothers provided milk samples during breastfeeding. During two of those sessions, they were given a nasal spray—either containing oxytocin or a placebo—in a randomized, double-blind design. The goal was to track changes in oxytocin levels in breast milk and to see how these levels corresponded with depressive symptoms.
Findings That Challenge Assumptions
One of the study’s most striking findings was, in a sense, what wasn’t found. Contrary to expectations, baseline oxytocin levels in breast milk did not differ significantly between mothers with and without depressive symptoms. This undermines the assumption that postnatal depression simply reflects a deficit in oxytocin production.
This doesn’t mean oxytocin plays no role in the challenges faced by depressed mothers. Far from it. When the nasal spray was administered, the plot thickened: only the non-depressed mothers showed a measurable increase in breast milk oxytocin. In mothers with depression, oxytocin levels remained flat—even with direct stimulation.
This asymmetry offers a compelling clue: the problem may not lie in the ability to produce oxytocin, but in the ability to respond to it.
A Disrupted Loop: Brain and Breast Out of Sync
So, what’s going wrong? The study’s authors propose a disruption in the communication pathway between the brain and the breast. Think of it as a broken feedback loop. In mothers without depression, oxytocin released in the brain enhances mood and bonding, while simultaneously prompting the body to release milk. The act of breastfeeding, in turn, reinforces oxytocin release—a virtuous cycle of physical and emotional nourishment.
In mothers with postnatal depression, this harmony appears to unravel. While milk production may remain intact—suggesting the peripheral oxytocin system is functional—the emotional component, regulated by the brain’s central oxytocin system, seems impaired. As a result, breastfeeding may become a mechanical act, stripped of its usual emotional rewards.
Kate Lindley Baron-Cohen explains it succinctly: “This indicates there may be a disruption in the brain-to-breast oxytocin pathway in mothers experiencing postnatal depression. It might explain why some mothers can lactate but do not experience the calming or bonding effects of breastfeeding.”
The Human Cost of Disconnection
The implications are more than academic. If breastfeeding no longer soothes the mother or strengthens attachment, it may start to feel like a burden rather than a bond. This can accelerate a cycle of emotional withdrawal, early weaning, and deepening depression—denying both mother and infant the psychological benefits that breastfeeding is known to provide.
Worse still, this breakdown in bonding could ripple across a child’s development. Secure attachment in infancy lays the groundwork for future emotional health. If oxytocin signaling is stunted early on, it might subtly influence how the child learns to connect with others.
Yet, as Baron-Cohen points out, these difficulties may not be rooted in hormonal failure alone. “Our findings suggest lactation difficulties in mothers with depression may be more psychological than biological,” she says. That nuance is crucial—because it means interventions don’t necessarily need to be chemical to be effective.
Toward Better Support and Smarter Treatments
One of the most encouraging takeaways from the study is the possibility of targeted intervention. If oxytocin responsiveness is blunted in the brain but not the body, could new treatments recalibrate the system?
There’s already growing interest in intranasal oxytocin as a potential treatment for a range of psychiatric disorders, including depression, PTSD, and autism. But this study suggests such treatments may not work uniformly—especially in mothers with postnatal depression. A more nuanced approach may be required.
Instead of viewing oxytocin simply as a hormone to be boosted, researchers may need to consider how the brain uses oxytocin. Enhancing receptor sensitivity, or synchronizing hormonal delivery with meaningful maternal-infant interaction, could be more effective than dosing alone.
Crucially, psychological therapies that address maternal stress, guilt, and social isolation may also help reset the oxytocin loop. If depression disrupts the rewarding experience of breastfeeding, then restoring joy—not just milk flow—should be the goal.
Limitations, But a Promising Path Forward
The study isn’t without its limitations. The sample size, though carefully selected, was modest. Breast milk contains only trace amounts of oxytocin, making precise measurement difficult. The timing of sample collection—once per session—provides only a snapshot of hormonal activity that may fluctuate with emotional and physiological states.
Still, the study represents a leap forward in understanding the intricate relationship between mood, hormones, and motherhood. And perhaps more importantly, it reframes the conversation around postnatal depression. Instead of seeing affected mothers as deficient or broken, it highlights a systemic disconnection—one that could be mended with the right support.
Baron-Cohen and her colleagues aren’t stopping here. “We’re continuing to investigate how oxytocin may influence the transference of mental health difficulties across development,” she says. That includes long-term studies that follow mothers and their children to see how these early hormonal dynamics shape emotional trajectories over time.
The Hidden Chemistry of Care
What this study ultimately reveals is that mother-infant bonding isn’t just a matter of love and instinct—it’s also physiology, and sometimes that physiology can fail to cooperate. Postnatal depression doesn’t make someone a bad mother. It interferes with the chemistry that’s supposed to help her feel like one.
In the end, oxytocin may be just one thread in a larger emotional tapestry, but it’s a vital one. When it flows freely, it weaves comfort, connection, and resilience. When it’s blocked or blunted, even the most natural acts—like holding, feeding, or gazing at your baby—can feel distant.
Understanding this disruption not only deepens our compassion for struggling mothers, but also opens the door to better treatments. It’s not enough to tell women to “just bond” or “try harder” to breastfeed. We must understand the biology beneath their struggle and meet them with science, support, and empathy.
Because sometimes, the hardest thing about being a mother isn’t the lack of love—but the lack of feeling it.