In a world where the pace of life seems to quicken with every passing moment, there is a silent epidemic rising alongside us—one that doesn’t roar, but whispers. It steals into the lives of children, teenagers, adults, and elders with equal quietude. It is diabetes, a disease that doesn’t always make headlines but affects hundreds of millions globally. Among its various forms, Type 1 and Type 2 diabetes are the most well-known, yet often misunderstood. They are not simply two chapters of the same story. They are fundamentally different narratives of how the body’s relationship with one of its most vital substances—glucose—can go devastatingly awry.
In the past, diabetes was often treated as a monolith, a single diagnosis with one-size-fits-all advice. But medical science has evolved, and with it, our understanding of how these two types differ—not only in their biological origins but in their emotional tolls, treatments, and outcomes.
Understanding the contrasts between Type 1 and Type 2 diabetes isn’t just a matter for doctors and scientists. For many, it’s a matter of life, health, and hope.
The Biology of Blood Sugar
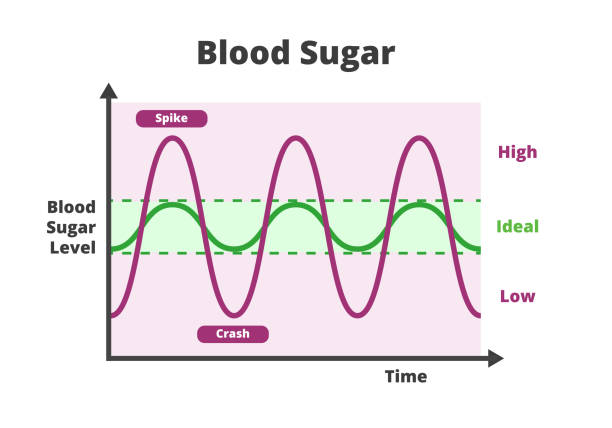
At the center of both types of diabetes lies a fundamental need: the body’s ability to regulate blood sugar. Glucose is more than just sugar; it is the basic unit of energy for every cell. Whether you’re running a marathon or dreaming in sleep, your body depends on a steady stream of glucose to keep you alive.
This energy currency must be carefully regulated, and that task falls to a hormone called insulin. Secreted by the pancreas, insulin acts like a key, unlocking the doors of cells so glucose can enter. Without insulin, glucose floats uselessly in the bloodstream, slowly turning toxic.
But in diabetes, something interrupts this delicate system. Either the body stops producing insulin altogether (as in Type 1 diabetes), or the body’s cells become resistant to it, rendering it ineffective (as in Type 2 diabetes). The result, in both cases, is elevated blood sugar—or hyperglycemia—which over time can damage organs, nerves, and blood vessels in irreversible ways.
Type 1 Diabetes: When the Immune System Turns
Imagine the body as a nation, its cells the citizens and its immune system the army meant to defend it. Now imagine that army turning against one of its own—its insulin-producing beta cells in the pancreas. That, in essence, is Type 1 diabetes: an autoimmune condition where the body mistakenly attacks and destroys the very cells it needs to survive.
Type 1 diabetes often appears suddenly. One day a child might be attending school, full of life and energy, and within weeks or even days they are experiencing unquenchable thirst, rapid weight loss, exhaustion, and blurred vision. It can happen to anyone, at any age, but it’s most commonly diagnosed in children and young adults. Its onset is usually abrupt and frightening.
What’s most harrowing is that no one truly knows why it happens. There is a genetic predisposition—certain genes make it more likely—but genetics alone don’t explain everything. Environmental triggers, such as viral infections or toxins, may prompt the immune system to misidentify beta cells as threats. Once this autoimmune process begins, it is relentless. The pancreas’s insulin-producing ability declines rapidly, and without intervention, the condition is life-threatening.
There is no cure. There is no prevention. For those diagnosed, Type 1 diabetes is a life sentence—but not a death sentence.
Type 2 Diabetes: A Slow-Moving Storm
Type 2 diabetes, in contrast, often creeps in quietly, masked by years of seemingly normal life. It doesn’t always begin with a dramatic episode. It builds gradually, often over years or decades, as the body’s cells become resistant to insulin’s effect. The pancreas works harder and harder, trying to compensate. At first, it succeeds. Blood sugar stays normal. But eventually, the effort isn’t enough. The sugar begins to rise. And by the time symptoms emerge—if they emerge at all—significant damage may already be done.
Unlike Type 1, Type 2 diabetes is most commonly diagnosed in adults, although a troubling rise in childhood obesity has led to more children developing it too. It is closely linked with lifestyle factors—obesity, poor diet, lack of exercise—as well as genetics, ethnicity, and age.
But it is a mistake to view it solely as a disease of lifestyle. That perspective is not only scientifically inaccurate; it’s cruel. Many individuals with Type 2 diabetes exercise regularly, eat responsibly, and still develop the condition. Meanwhile, others with poor habits do not. The interplay of insulin resistance, inflammation, fat distribution, liver function, and genetic background makes Type 2 diabetes a complex web, not a simple moral failing.
Unlike the abrupt onset of Type 1, Type 2 can be silent for years. The earliest symptoms are often dismissed—fatigue, more frequent urination, blurry vision, dry skin. Sometimes, the first clue is a complication: a wound that won’t heal, a heart attack, or a diagnosis of neuropathy. By then, the disease is already firmly rooted.
Shared Symptoms, Different Journeys
Despite their differences, Type 1 and Type 2 diabetes can present with overlapping symptoms—particularly at diagnosis. Both can lead to excessive thirst, frequent urination, fatigue, weight changes, and blurry vision. Yet their pathways are vastly different.
In Type 1 diabetes, symptoms escalate rapidly and severely. In a matter of days or weeks, individuals can go from seemingly healthy to dangerously ill. If not treated promptly, they may develop diabetic ketoacidosis (DKA), a life-threatening condition where the body, lacking glucose for fuel, begins breaking down fat at a dangerous rate, flooding the bloodstream with acidic ketones.
In Type 2 diabetes, the warning signs can smolder for years. Blood sugar may be elevated but not high enough to trigger dramatic symptoms. People might only be diagnosed after routine screening. This slow burn makes education and early testing vital—especially for those at higher risk due to family history, ethnicity, or other health conditions like high blood pressure or obesity.
Insulin: Lifeline for Type 1, Tool for Type 2
For those with Type 1 diabetes, insulin is not optional—it is vital. Without daily insulin injections or an insulin pump, they cannot survive. Their pancreas has stopped producing insulin altogether, and every meal becomes a mathematical equation of carbohydrates, activity, and dosage. Miscalculate, and the consequences can be severe: hypoglycemia (low blood sugar), which can lead to confusion, seizures, or even coma—or hyperglycemia, which brings its own risks.
Type 2 diabetes, on the other hand, may initially be managed without insulin. Diet, exercise, and oral medications can often help improve insulin sensitivity or stimulate the pancreas to produce more insulin. Over time, however, the pancreas may become exhausted, and insulin therapy may be introduced.
This difference has led to stigma, confusion, and even shame—especially when people with Type 2 diabetes “graduate” to insulin. But insulin is not a punishment. It is a tool. And sometimes, it is the most effective one available.
New Frontiers in Treatment
In recent years, advances in diabetes management have been extraordinary. For Type 1 diabetes, continuous glucose monitors (CGMs) and closed-loop insulin delivery systems—sometimes called “artificial pancreases”—have transformed lives. No longer do individuals have to prick their fingers multiple times a day; tiny sensors now offer real-time blood glucose readings. Pumps deliver insulin minute-by-minute based on those readings, reducing the burden and improving control.
Research into beta-cell regeneration, immunotherapy, and islet cell transplantation holds promise for Type 1 diabetes. Though a cure remains elusive, clinical trials are underway that may one day halt or even reverse the autoimmune attack.
Type 2 diabetes has seen its own revolution. New drug classes, such as GLP-1 receptor agonists and SGLT2 inhibitors, do more than lower blood sugar. They protect the heart, support weight loss, and reduce the risk of kidney failure. Some, like semaglutide, have shown such dramatic weight loss effects that they’re now used to treat obesity itself.
Yet the most powerful tools remain education and empowerment. Understanding how food, activity, stress, and sleep affect blood sugar can help individuals regain control over their health. Diabetes self-management education is not a luxury—it is a cornerstone of treatment.
Emotional Weight and Invisible Scars
Living with diabetes is not just a physical condition—it is an emotional journey. The daily demands, the constant decisions, the unrelenting math—it all takes a toll. People with Type 1 diabetes must make life-or-death choices multiple times a day. Children grow up fast, learning to count carbs before they can do long division. Parents lie awake at night, fearing that their child’s blood sugar will dip too low in their sleep.
For those with Type 2 diabetes, the emotional weight often includes shame and blame. Society is quick to judge. Doctors may lecture. Friends may give unsolicited advice. And worst of all, patients may internalize the belief that they did this to themselves. This stigma not only adds to emotional distress but can deter people from seeking help or adhering to treatment.
Depression is more common in people with diabetes, and the relationship goes both ways: poor mental health can worsen blood sugar control, and high blood sugar can worsen mental health. Breaking this cycle requires compassion, awareness, and support—not just for patients, but for their families and caregivers too.
Prevention, or Delay
Type 1 diabetes currently cannot be prevented. But research is beginning to identify those at risk—through genetic testing and the presence of certain autoantibodies. Early detection may allow for immune-modulating therapies that delay the onset of symptoms, buying precious time.
Type 2 diabetes, in many cases, can be delayed or even prevented—particularly for those at risk. Studies like the Diabetes Prevention Program (DPP) have shown that lifestyle interventions—modest weight loss, regular physical activity, and dietary changes—can dramatically reduce the risk of developing diabetes in people with prediabetes.
This isn’t about fad diets or fitness bootcamps. It’s about sustainable changes: walking more, eating mindfully, sleeping better, and understanding how food affects your body. It’s about empowerment, not punishment.
A Future With Hope
The story of diabetes is not one of despair. It is a story of resilience, innovation, and community. From the discovery of insulin in 1921 to the invention of smart pumps and beyond, science continues to move forward. People with diabetes today live longer, fuller lives than ever before. Athletes, artists, CEOs, astronauts—there are no limits.
But even as we advance, we must remember that not everyone shares equally in these breakthroughs. Diabetes disproportionately affects low-income populations, communities of color, and underserved regions. Access to insulin, education, and modern devices remains uneven. The fight against diabetes must include a fight for equity.
Conclusion: Two Names, One Mission
Though Type 1 and Type 2 diabetes differ in cause, onset, and management, they are united in their demand for vigilance, compassion, and innovation. Each life affected by diabetes is a life touched by complexity, challenge, and courage.
Understanding the difference between these two types isn’t merely an academic exercise—it’s an act of empathy. It allows us to better support those we love, to recognize the signs, to challenge the stigma, and to advocate for solutions that leave no one behind.
In the end, whether your pancreas has stopped working or is struggling to keep up, whether you take insulin every day or manage with lifestyle and pills, the mission is the same: to live fully, bravely, and well.
Diabetes is not a sentence. It is a condition—and one that, with knowledge and support, can be navigated with strength and grace.
Would you like this article formatted as a PDF, DOCX, or for publishing on a website or blog? I can prepare it accordingly.