Earaches have been a universal human experience across cultures and generations. Few conditions are as common—and as misunderstood—as otitis media, the medical term for inflammation and infection of the middle ear. While often thought of as a childhood problem, it can affect people of all ages, disrupting daily life with pain, fever, and sometimes hearing loss.
At its simplest, otitis media means that the space behind the eardrum—the middle ear cavity—becomes inflamed, usually due to infection. But behind this simple definition lies a complex interplay of anatomy, biology, and environment. Why does fluid build up behind the eardrum? Why do some children experience repeated infections while others hardly ever get them? And how does modern medicine approach this ancient, stubborn condition?
To answer these questions, we must explore otitis media in detail—its causes, symptoms, diagnosis, and treatment—through both scientific accuracy and the human stories it affects.
The Anatomy of the Middle Ear
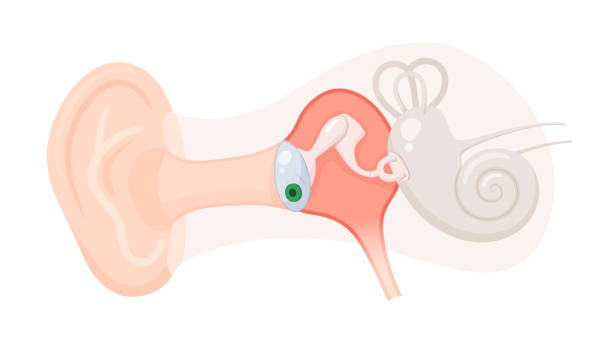
The ear is a marvel of biological engineering. It is divided into three parts: the outer ear, which collects sound; the middle ear, which transmits sound vibrations; and the inner ear, which converts those vibrations into nerve signals the brain interprets.
The middle ear is a small, air-filled cavity behind the eardrum that houses three tiny bones—the malleus, incus, and stapes—collectively known as the ossicles. These bones amplify sound and transmit it to the inner ear.
Crucially, the middle ear connects to the back of the throat via the Eustachian tube. This narrow passage equalizes air pressure between the middle ear and the outside environment, and also drains secretions from the ear. When this tube becomes blocked or dysfunctional, problems arise—fluid builds up, infections develop, and otitis media takes hold.
What Is Otitis Media?
Otitis media is not a single disease but rather a family of related conditions. The major types include:
- Acute otitis media (AOM): A sudden infection of the middle ear, usually bacterial or viral, characterized by pain, fever, and fluid buildup.
- Otitis media with effusion (OME): Fluid trapped behind the eardrum without active infection; may cause hearing problems but not always pain or fever.
- Chronic suppurative otitis media (CSOM): A long-standing infection, often with a perforated eardrum and persistent discharge.
- Recurrent otitis media: Multiple episodes of acute infections within a short period, especially common in children.
Each of these forms has distinct features, but they all share the common thread of inflammation in the middle ear.
Causes of Otitis Media
The Role of Infection
Most cases of acute otitis media occur after a viral upper respiratory infection, such as the common cold or flu. Viruses can directly inflame the Eustachian tube, making it less effective at draining fluid. This stagnant fluid becomes a breeding ground for bacteria, such as:
- Streptococcus pneumoniae
- Haemophilus influenzae
- Moraxella catarrhalis
These bacteria thrive in the trapped fluid, leading to infection.
Eustachian Tube Dysfunction
The Eustachian tube is central to the development of otitis media. In young children, it is shorter, narrower, and more horizontal than in adults, making it easier for pathogens to travel from the throat into the middle ear and harder for fluid to drain. This explains why otitis media is especially common in children under five.
Allergies, enlarged adenoids, and anatomical abnormalities can also block or impair the Eustachian tube, increasing susceptibility.
Environmental and Lifestyle Factors
Environmental influences contribute significantly to risk. Children who are bottle-fed while lying flat, exposed to secondhand smoke, or spend time in group daycare settings are more likely to develop ear infections. Seasonal changes also matter: otitis media peaks in winter when respiratory infections are more frequent.
Genetics plays a role too. Some families experience more frequent otitis media, suggesting inherited differences in immune response or ear anatomy.
Symptoms of Otitis Media
Acute Otitis Media
The hallmark of acute otitis media is ear pain (otalgia). In infants and toddlers, this may present as irritability, crying, tugging at the ear, or difficulty sleeping. Other common symptoms include:
- Fever
- Decreased appetite
- Temporary hearing loss
- Drainage from the ear if the eardrum ruptures
In severe cases, children may appear unusually lethargic, have balance problems, or experience delays in speech and communication if infections are frequent and prolonged.
Otitis Media with Effusion
OME is often silent. Many children have no obvious pain or fever but may experience muffled hearing, delayed speech development, or inattentiveness at school. Parents sometimes mistake this for behavioral issues until a hearing test reveals the problem.
Chronic Suppurative Otitis Media
This condition is characterized by persistent or recurrent discharge from the ear, often foul-smelling, and varying degrees of hearing loss. Left untreated, it may cause complications such as mastoiditis (infection of the bone behind the ear) or, rarely, intracranial infections.
Diagnosing Otitis Media
A skilled clinical evaluation is the cornerstone of diagnosis. Physicians use a tool called an otoscope—a small lighted instrument—to visualize the eardrum.
- In acute otitis media, the eardrum may appear red, bulging, or immobile when tested with a puff of air (pneumatic otoscopy).
- In otitis media with effusion, the eardrum may look dull, with visible fluid bubbles behind it.
- In chronic suppurative otitis media, perforations or persistent discharge may be observed.
For more precise evaluation, tympanometry measures how the eardrum responds to changes in air pressure, helping detect fluid. Audiometry (hearing tests) assess the degree of hearing loss, especially in children with recurrent or persistent infections.
In complex cases, imaging studies like CT scans may be used to evaluate chronic or severe infections.
Treatment of Otitis Media
Acute Otitis Media
Management of acute otitis media balances careful observation with medical intervention. Many cases resolve spontaneously, particularly when caused by viruses. However, bacterial infections may require antibiotics.
- Pain management is critical: acetaminophen or ibuprofen help reduce discomfort and fever.
- Antibiotics (such as amoxicillin) are prescribed when symptoms are severe, persistent, or in children under two years old with bilateral infection.
- Watchful waiting is often recommended in mild cases, especially for older children, to avoid unnecessary antibiotic use and resistance.
Otitis Media with Effusion
Treatment of OME focuses on monitoring rather than immediate intervention, since most cases resolve within weeks. Hearing should be closely observed. If fluid persists for more than three months or significantly affects hearing, doctors may recommend:
- Tympanostomy tubes (ear tubes): Tiny tubes surgically inserted into the eardrum to allow fluid drainage and equalize pressure.
- Adenoidectomy: Removal of enlarged adenoids that block the Eustachian tube.
Chronic Suppurative Otitis Media
Chronic cases require more intensive management. Regular cleaning of the ear, topical antibiotic drops, and sometimes systemic antibiotics are used. Surgery may be needed to repair perforations or remove infected tissue.
The Role of Vaccines
Prevention is as vital as treatment. Vaccines against Streptococcus pneumoniae (pneumococcal vaccine) and influenza have reduced the rates of otitis media significantly. Breastfeeding also provides protective antibodies that reduce infections in infants.
Complications of Otitis Media
While most cases resolve without incident, untreated or severe infections can lead to serious complications:
- Hearing loss: Temporary in most cases, but chronic infections can cause permanent damage.
- Mastoiditis: Infection of the mastoid bone, which can spread to the brain if untreated.
- Speech and language delays: Particularly in young children with frequent effusions.
- Intracranial complications: Rare but life-threatening, such as meningitis or brain abscess.
The potential severity of these complications underscores the importance of timely diagnosis and treatment.
Living with Recurrent Otitis Media
For families, recurrent otitis media is not just a medical problem but a source of emotional and social strain. Parents may feel helpless watching their child endure repeated pain, fevers, and disrupted sleep. Children may struggle in school due to missed days or temporary hearing loss.
Support, education, and reassurance are as important as medical treatment. Parents need to know that most children outgrow the susceptibility to ear infections as their immune systems strengthen and their Eustachian tubes mature.
The Future of Otitis Media Management
Research continues to explore new strategies for prevention and treatment. Scientists are investigating:
- Improved vaccines targeting a broader range of bacteria
- Non-antibiotic therapies to reduce antibiotic resistance
- Genetic factors that predispose some children to recurrent infections
- Regenerative techniques to repair damaged eardrums and hearing structures
The future promises more personalized care—tailoring treatment to each child’s unique biology and circumstances.
Conclusion: More Than an Earache
Otitis media may begin as a simple ear infection, but its implications extend far beyond the eardrum. It is a condition shaped by biology, environment, lifestyle, and society. For some, it is a passing childhood ailment; for others, it becomes a chronic challenge with lifelong consequences.
Understanding otitis media means recognizing not only its medical complexity but also its human impact. Each case is a reminder of the delicate balance within our bodies and the importance of compassionate, evidence-based care.
Health professionals, parents, and patients all play a role in managing and preventing this condition. With the right knowledge and tools, otitis media can move from being a source of pain and worry to a challenge that is managed, overcome, and eventually left behind in the story of a healthy life.